
Triptan & SSRI Compatibility Checker
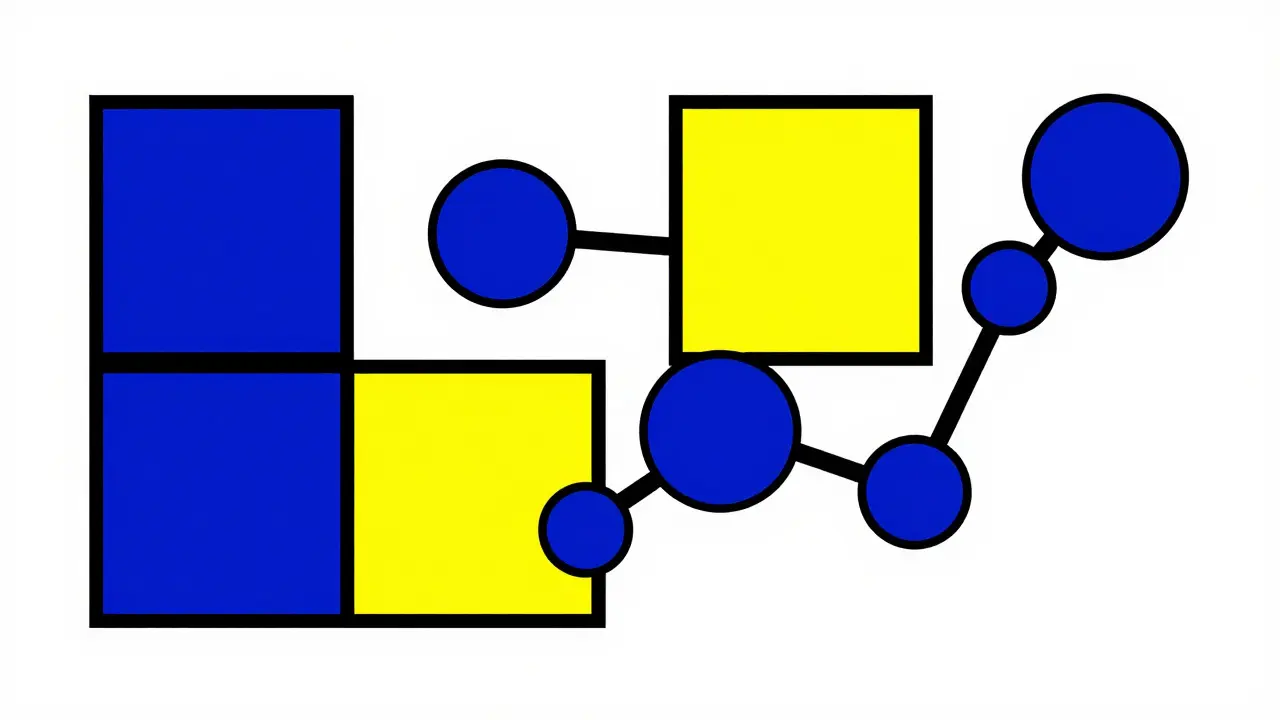
Why? The "Lock and Key" Mechanism
Triptans
Targets: 5-HT1B / 5-HT1D
Vasoconstriction KeysNo Mismatch
Serotonin Syndrome
Requires: 5-HT2A Stimulation
Dangerous Lock*Triptans lack the chemical "keys" to trigger serotonin toxicity locks.
While the combination is generally safe, awareness is key. Click any symptom you experience.
- Tremors or Twitching
- Shivering or Rigidity
- Excessive Sweating
- Rapid Heart Rate
- Confusion or Agitation
You might be sitting there holding your migraine pill prescription, feeling frustrated because the pharmacist hesitated before handing it over. They warned you about the combination, pointing to a decades-old caution flag. It happens often. Millions of people take selective serotonin reuptake inhibitors (SSRIs) for depression or anxiety. Many of those same people also struggle with migraines. For years, doctors and pharmacists were told not to mix these two essential treatments. But here is the reality that has been slowly emerging over the last twenty years: the danger was largely theoretical, not real.
The Origin of the Warning
To understand where we stand today, we have to look back at the decision made in 2006. The U.S. Food and Drug Administration issued a safety announcement regarding triptans and antidepressants. This created a ripple effect across the healthcare system. Approximately thirty-seven million Americans using SSRIs suddenly faced restrictions. The warning suggested a risk of serotonin syndrome, a condition caused by too much serotonin activity in the brain. At the time, the precaution made sense based on simple chemistry. Both drugs affect serotonin. Therefore, logically, combining them should increase levels further.
However, clinical reality did not match the theory. Over the years since that announcement, researchers began collecting actual data instead of relying on theoretical models. Dr. P. Ken Gillman, writing in the Headache Journal is a peer-reviewed publication for headache specialists., reviewed this issue extensively. He concluded there was neither significant clinical evidence nor theoretical reason to suspect serious serotonin syndrome from these combinations. Despite this, the warning stuck in many pharmacy software systems for nearly two decades.
Anatomy of the Drugs
We need to understand how these medications actually work to see why the alarm was raised. Triptans are a class of medication developed in the early 1990s for acute migraine treatment. Examples include sumatriptan, rizatriptan, and eletriptan. They function primarily as agonists at specific serotonin receptors, specifically the 5-HT1B is a serotonin receptor subtype targeted by triptans for vasoconstriction. and 5-HT1D. These receptors sit on blood vessels and nerve endings in the brain.
On the other side of the equation, you have SSRIs like fluoxetine (Prozac). These were introduced in the late 1980s. Their job is different. They inhibit the reuptake of serotonin, meaning they keep serotonin available in the synaptic cleft for longer. While this helps stabilize mood, it does raise overall serotonin levels. That is where the fear originated. If you increase serotonin availability while activating receptors, could you cause a storm? That was the hypothesis behind serotonin syndrome.
Why the Mechanism Matters
This is where the science gets fascinating. Serotonin syndrome requires overstimulation of specific receptors to trigger dangerous symptoms. Most research indicates that the 5-HT2A is the primary serotonin receptor implicated in serotonin syndrome pathogenesis. plays the leading role. Some involvement of the 5-HT1A receptor might also occur. Here is the catch: Triptans have very low affinity for 5-HT2A receptors. They barely touch them.
Think of it like a lock and key system. Triptans carry keys that fit specific locks (5-HT1B and 5-HT1D) that control blood vessel constriction. Serotonin syndrome happens when keys jam the locks responsible for motor control and autonomic stability (5-HT2A). Since triptans do not possess the right keys for those dangerous locks, the risk remains incredibly low. This receptor specificity explains why the theoretical concern never materialized in patient populations. Experts like Dr. David M. Perloff noted in his reviews that plausibility was doubted precisely because of this receptor mismatch.
Clinical Evidence and Real Data
If we move beyond theory to hard numbers, the picture becomes clear. A massive study published in JAMA Neurology in 2019 analyzed data from over 61,000 patients treated at a major medical center between 1990 and 2018. The goal was to find confirmed cases of serotonin syndrome among migraine patients taking both triptans and SSRIs or SNRIs. The result was zero. Not one case met the diagnostic criteria. This contradicted the assumption that the combination creates a significant spike in risk compared to using an SSRI alone.
| Study Source | Year | Finding | Risk Level |
|---|---|---|---|
| JAMA Neurology (Buse et al.) | 2019 | 0 cases in 61,029 patients | Negligible |
| Gillman Review | 2010 | No clinical evidence found | Unsupported |
| American Migraine Foundation Survey | 2022 | 42% patients denied treatment | Burden High |
| IQVIA Prescription Audit | 2022 | Prescribing increased to 32.4% | Safety Confidence |
The data suggests that the FDA's 2006 warning affected patients unnecessarily. The estimated cost to the healthcare system was around $450 million annually due to patients switching to less effective or more expensive treatments. Instead of using a highly effective triptan, patients were pushed toward alternatives that worked slower or had higher costs. We are talking about millions of people who suffered through preventable pain because of a safety guideline built on precaution rather than proof.
Impact on Patient Care
The effects of this warning went beyond statistics; they touched lives directly. Surveys from organizations like the Migraine Foundation of New Zealand highlighted how common it is for patients to hear they cannot take a triptan because they are on an antidepressant. In Reddit discussions from March 2023, users shared stories of pharmacists refusing to dispense the medication. Even if the pharmacist allowed it, the doctor might have hesitated. The psychological barrier is just as damaging as the physical restriction.
Approximately thirty to fifty percent of migraine patients also experience depression or anxiety. Treating both conditions is vital for quality of life. Denying the best option for migraine relief compromises their recovery. A 2022 survey showed forty-two percent of respondents reported being denied prescriptions. None of them had actually experienced serotonin syndrome. This highlights a disconnect between policy and patient outcomes. By 2024, educational efforts were underway to correct this misinformation, with quizzes explicitly teaching that the toxicity risk is false when co-prescribed.
Current Medical Consensus
As of 2026, the landscape has shifted significantly. The American Headache Society released a consensus statement in 2022 recommending clinicians should not avoid prescribing triptans to patients taking SSRIs. Major medical centers like the Mayo Clinic updated their position in 2023, stating the theoretical risk has not materialized in clinical practice. The European Medicines Agency never issued a similar warning, recognizing the lack of clinical evidence from the start.
Despite this progress, change is slow. Some pharmacy software systems still trigger alerts based on the 2006 data. Doctors need to advocate for their patients here. They can explain the receptor specificity to the pharmacist or override the alert with documentation. The trend in prescribing has already moved forward. Between 2007 and 2022, concurrent use rose from eighteen point seven percent to thirty-two point four percent. Clinicians are gaining confidence as the evidence base solidifies.
Managing the Conversation
If you are navigating this as a patient, preparation helps. Know your medication names. Carry a list of what you take. If a pharmacist raises concerns, ask about the specific mechanism. Mentioning the JAMA study or the American Headache Society guidelines can be helpful. Remember, the FDA label for sumatriptan was updated in 2023. It includes the warning but adds that epidemiological studies have not shown increased risk. Acknowledging this nuance matters.
Monitoring is still good practice. Any time you combine strong medications, awareness pays off. Watch for signs like tremors, confusion, fever, or agitation. These are classic symptoms of serotonin toxicity, though again, extremely rare in this combo. Most doctors agree that routine monitoring isn't required anymore, but basic vigilance ensures safety.
Can I safely take my migraine med with my antidepressant?
Yes, current evidence supports safe co-prescription. Large scale studies show no increase in serotonin syndrome risk for the typical patient.
Why did the FDA issue a warning in 2006?
The warning was based on theoretical pharmacology suggesting serotonin overload, not on actual adverse event reports in patients.
What are the symptoms of serotonin syndrome I should watch for?
Look for muscle twitching, shivering, sweating, high heart rate, confusion, or agitation. Seek help immediately if these occur.
Does every SSRI interact the same way?
All SSRIs work similarly, but individual responses vary. Always consult your provider regarding your specific regimen.
Will my insurance cover the combination?
Coverage depends on your plan, but clinical consensus now favors approving these combinations without prior authorization hurdles.