MS Vision Symptom Checker
This tool helps you understand how your vision symptoms might relate to multiple sclerosis. Based on your input, it will provide information about potential causes and next steps.
Select Your Symptoms
Potential MS-Related Vision Issue
Next Steps
When you hear the word "sclerosis," you probably think of muscle stiffness or joint pain. But for many people, the biggest surprise is how the condition can mess with your eyesight. If you’ve been diagnosed with Multiple sclerosis is a chronic autoimmune disease that attacks the protective coating of nerve fibers in the central nervous system. This damage disrupts the flow of electrical signals, leading to a wide range of symptoms, including vision problems. In this guide we’ll break down exactly how multiple sclerosis vision loss shows up, why it happens, and what you can do to protect your eyes.
Key Takeaways
- Up to 80% of people with multiple sclerosis experience some form of visual disturbance.
- The most common eye issue is optic neuritis, an inflammation of the optic nerve that can cause pain and temporary loss of sight.
- Modern imaging tools like OCT (optical coherence tomography) can detect subtle nerve fiber loss before you notice any symptoms.
- Early treatment with disease‑modifying therapy (DMT) reduces the risk of permanent visual damage.
- Simple lifestyle tweaks-regular eye exams, protective eyewear, and eye‑friendly diet-support long‑term eye health.
How Multiple Sclerosis Affects the Visual System
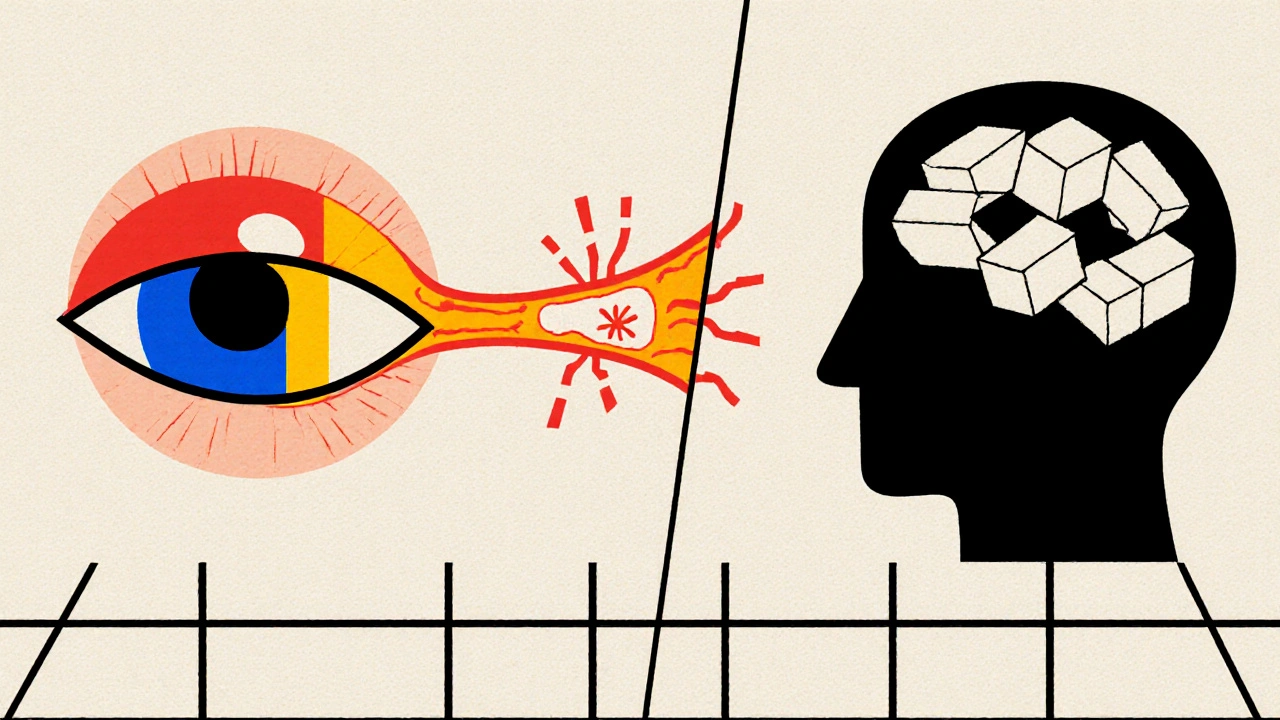
To understand why vision gets hit, you need to picture the eye’s connection to the brain. Light enters the retina, converts into electrical signals, and travels via the optic nerve to the visual cortex. In multiple sclerosis, the immune system mistakenly attacks myelin-the insulating layer around that optic nerve. When myelin is damaged, signal transmission slows or stops, leading to blurry vision, double vision, or even temporary blind spots.
Beyond the optic nerve, MS can involve other parts of the visual pathway:
- Optic chiasm and tract: Demyelination here can cause visual field deficits that affect both eyes.
- Visual cortex: Lesions may produce visual hallucinations or difficulty recognizing objects.
- Extra‑ocular muscles: Inflammation of the nerves that control eye movement can create diplopia (double vision) and misalignment.
Because the central nervous system is a single network, any flare‑up can potentially impact one or several visual structures at once.
Common Visual Symptoms in MS
Not everyone gets the same eye problems, but a handful of symptoms show up repeatedly. Below is a quick reference table that ranks them by how often they occur.
| Symptom | Typical Onset | Prevalence (%) | Potential Long‑Term Impact |
|---|---|---|---|
| Optic neuritis | Acute, often first sign | 55‑65 | Usually reversible, but can leave residual scotoma |
| Diplopia (double vision) | During relapses affecting cranial nerves III, IV, VI | 30‑40 | May become permanent if extra‑ocular muscle control is lost |
| Reduced visual acuity | Gradual or acute | 20‑30 | Can be permanent if retinal nerve fiber layer thins |
| Visual field defects (e.g., altitudinal loss) | Often subtle, detected by testing | 15‑25 | May become stable or progress based on lesion location |
| Nystagmus (involuntary eye movement) | Variable, linked to brainstem lesions | 10‑15 | Usually mild, but can affect reading |
These numbers come from a 2023 multinational cohort of 2,800 MS patients, summarizing both relapsing‑remitting and progressive forms.
Diagnosing Vision Problems in MS
When you report any visual change, your neurologist will likely refer you to a neuro‑ophthalmologist. The exam often includes:
- Visual acuity test: Standard eye‑chart assessment.
- Visual field testing: Automated perimetry maps blind spots.
- Colour vision test: Detects subtle optic nerve dysfunction.
- Fundoscopic exam: Direct view of the optic disc for swelling.
- Optical coherence tomography (OCT) measures the thickness of the retinal nerve fibre layer (RNFL). Thinning of the RNFL is a reliable marker of past optic neuritis episodes, even when vision feels normal.
Magnetic resonance imaging (MRI) of the brain and orbits helps confirm active inflammation. Gadolinium‑enhancing lesions on the optic nerve are a hallmark of acute optic neuritis.
Treating and Managing Vision Issues
There are two fronts in treatment: addressing the underlying MS activity and handling the eye symptom itself.
1. Disease‑Modifying Therapies (DMTs)
High‑efficacy DMTs such as ocrelizumab, natalizumab, and the newer sphingosine‑1‑phosphate receptor modulators (e.g., ozanimod) dramatically cut relapse rates. Studies show that patients on effective DMTs have a 40‑50% lower risk of developing new optic neuritis episodes.
2. Acute Optic Neuritis Management
- Corticosteroids: Intravenous methylprednisolone (1 g daily for 3‑5 days) speeds recovery but doesn’t affect final visual outcome.
- Plasma exchange: Considered for steroid‑refractory cases; can restore vision in up to 30% of severe attacks.
3. Symptom‑Specific Interventions
- Prism glasses: Realign images for patients with persistent diplopia.
- Low‑vision aids: Magnifiers, high‑contrast reading materials, and screen‑reading software help when visual acuity stays reduced.
- Eye‑movement therapy: Vision‑rehabilitation exercises improve tracking and reduce nystagmus impact.
4. Lifestyle and Protective Measures
Even with medication, daily habits matter:
- Regular eye exams: At least once a year, or sooner after any flare‑up.
- UV protection: Sunglasses with UV‑400 filter reduce retinal stress.
- Omega‑3‑rich diet: Fish oil and flaxseed support myelin health.
- Manage blood pressure and diabetes: Both conditions can worsen microvascular eye damage.

Living with Vision Changes: Practical Tips
Adjusting your environment makes a huge difference. Here are some quick hacks:
- Use large‑print keyboards and increase screen font size to 150‑200%.
- Install bright, non‑glare lighting-LEDs with a color temperature around 5000 K work well.
- Organize home objects consistently; a clutter‑free layout reduces reliance on peripheral vision.
- Try high‑contrast settings on smartphones (dark mode with yellow text is easier on the eyes for many).
- If you drive, schedule regular vision checks and consider a bi‑optic driving assessment after any optic neuritis episode.
Frequently Asked Questions
Can multiple sclerosis cause permanent blindness?
Permanent blindness is rare. Most visual episodes, especially optic neuritis, recover fully or leave only minor blind spots. Prompt treatment and early DMT use dramatically lower the chance of lasting damage.
How quickly should I see a doctor if I notice sudden vision loss?
Within 24 hours. Acute optic neuritis can worsen quickly, and early steroids improve recovery speed.
Is OCT safe for regular monitoring?
Yes. OCT uses harmless light waves and takes a few seconds per eye. It’s now standard for tracking RNFL thinning in MS clinics.
Do low‑vision aids replace the need for glasses?
Not usually. Low‑vision aids complement prescription glasses when acuity remains low despite correction.
Can lifestyle changes slow eye involvement?
While lifestyle can’t stop demyelination, controlling blood pressure, maintaining a healthy weight, and protecting eyes from UV light reduce secondary damage and improve overall visual comfort.
Vision problems in multiple sclerosis are often the first sign that the disease is active. By recognizing symptoms early, using modern imaging, and staying on effective disease‑modifying therapy, most people keep their sight and maintain a high quality of life. Keep the conversation open with your neurologist and eye specialists-you’re part of a team that can safeguard both your brain and your eyes.
Comments (14)
Sarah Riley
October 22, 2025 AT 16:45
The optic neuritis cascade is a classic demyelination feedback loop that most patients ignore until vision fails.
Tammy Sinz
October 26, 2025 AT 03:05
Acute visual disturbances in MS serve as a barometer for disease activity, signalling that inflammatory processes have breached the optic pathway. Early detection via OCT can pinpoint subtle retinal nerve fiber layer thinning before the patient perceives any deficit. Prompt initiation of high‑efficacy DMTs has been shown to slash relapse rates, preserving both neural integrity and visual acuity. Moreover, integrating regular neuro‑ophthalmologic assessments into your care plan creates a proactive safety net against irreversible retinal damage.
Christa Wilson
October 29, 2025 AT 14:25
Seeing the light at the end of the tunnel is totally possible! 😊 Keep those eye exams on schedule and trust that modern therapies are on your side. 🌟
John Connolly
November 2, 2025 AT 01:45
The visual axis is uniquely vulnerable in multiple sclerosis due to its reliance on tightly myelinated axons.
Their demyelination causes conduction velocity to drop, producing transient blurring or scotomas.
Corticosteroid infusion during acute optic neuritis accelerates symptom resolution, typically within days.
However, steroids do not alter the ultimate visual outcome, underscoring the importance of disease‑modifying therapy.
High‑potency agents such as ocrelizumab or natalizumab have demonstrated a 40 % reduction in new optic neuritis events.
Regular optical coherence tomography scans act as a quantitative biomarker, charting retinal nerve fiber layer loss over time.
Patients who maintain an RNFL thickness above 80 µm seldom experience permanent visual field deficits.
Lifestyle interventions-adequate omega‑3 intake, UV‑blocking eyewear, and blood pressure control-mitigate secondary vascular insults.
Prism glasses can realign images for those left with persistent diplopia, improving binocular function without surgery.
Low‑vision aids, including high‑contrast reading tools and screen magnifiers, restore functional independence for residual acuity loss.
Vision‑rehabilitation exercises target nystagmus and saccadic tracking, fostering smoother eye movements.
The multidisciplinary team-neurologist, neuro‑ophthalmologist, and low‑vision specialist-should convene whenever a visual flare is reported.
Driving assessments post‑optic neuritis are prudent, as reaction time may be subtly compromised despite recovered acuity.
In sum, early recognition, aggressive immunotherapy, and vigilant ocular monitoring converge to safeguard sight.
Maintaining open communication with your care providers empowers you to navigate the visual challenges of MS with confidence.
Suryadevan Vasu
November 5, 2025 AT 13:05
Demyelination slows signal transduction, leading to intermittent blurring; timely OCT can capture early axonal loss.
Vin Alls
November 9, 2025 AT 00:25
The eye’s highway gets jammed when the myelin coat peels off, turning crisp pictures into watercolor smudges. A swift steroid drip acts like a traffic cop, clearing the congestion for a smoother ride. Meanwhile, cutting‑edge DMTs are the road crews that repave the lanes, preventing future pile‑ups. Pair that with antioxidant‑rich foods, and you’ve got a scenic route back to visual clarity.
Tiffany Davis
November 12, 2025 AT 11:45
Consistent annual eye exams coupled with protective sunglasses form a low‑maintenance strategy to monitor and guard against progressive optic damage.
Don Goodman-Wilson
November 15, 2025 AT 23:05
Oh sure, just ignore the flashing lights and hope your optic nerve decides to behave-you'll probably end up starring in a blackout documentary.
Bret Toadabush
November 19, 2025 AT 10:25
They don't tell u that the pharma companies are pushin' these fancy scans just to make more monee, but u know the truth-big data = big control.
Diane Thurman
November 22, 2025 AT 21:45
Honestly, if you don't follow the doctor reccommendations, u might as well just quit and hope for the best… lol.
Iris Joy
November 26, 2025 AT 09:05
You've got this! Prioritizing regular OCT checks and staying on a solid DMT plan will give your eyes the best shot at staying sharp. Remember, every small healthy habit adds up to big protection.
Emma Parker
November 29, 2025 AT 20:25
Totally feel you, Christa! Even a quick blink of an eye exam can catch issues before they snowball-keep that optimism rolling.
Emily Collins
December 3, 2025 AT 07:45
The depth of your breakdown really paints the full picture; while the facts are stark, they also illuminate a clear path forward.
Harini Prakash
December 6, 2025 AT 19:05
Great points, Tammy! Your emphasis on early detection and integrated care really hits home. 😊👍